Medical coding has always been complex — thousands of ICD-10 and CPT codes, frequent payer rule updates, and zero room for billing errors. For years, Computer-Assisted Coding (CAC) has helped organizations manage this complexity by suggesting codes for human review.
But suggesting codes is not the same as processing them. As coding volumes grow and coder shortages worsen, the need for full automation has become clear.
Autonomous medical coding goes further than CAC; it assigns, validates, and submits codes without manual intervention. In 2026, healthcare organizations are actively evaluating whether CAC is still enough.
This blog breaks down the key differences between the two, where each fits, and what to consider before making a change.
What Is Computer-Assisted Coding (CAC)?
Computer-Assisted Coding (CAC) uses natural language processing and machine learning algorithms to analyze clinical documentation and suggest appropriate medical codes. It was built to make coders faster — not to replace them. CAC systems typically fall into two types: structured input systems that use templates and rule-based logic, and unstructured input systems that use NLP to process free-text clinical notes.
Think of CAC as a digital co-pilot for medical coders. It scans clinical notes, identifies key diagnoses and procedures, and suggests matching codes — but a human coder still reviews and validates every suggestion before submission.
Early CAC systems were largely rule-based — relying on predefined keyword lists and logic trees to map clinical terms to codes. While effective for simple, repetitive encounters, rule-based systems struggled with complex documentation, abbreviations, and context-dependent clinical language. Modern CAC evolved to incorporate NLP and ML to handle this complexity — but the human approval dependency remained.
How CAC works, step by step:
- Clinical documentation is fed into the system (physician notes, discharge summaries, lab reports)
- NLP engine reads and interprets the unstructured text
- Rule-based logic and ML models identify diagnoses, procedures, and relevant clinical terms
- System suggests ICD-10 and CPT codes based on identified terms
- A coder reviews, adjusts if needed, and approves
- Final codes are submitted to the billing system
CAC meaningfully improved coding speed and reduced manual lookup time. However, human oversight is still required; coders often evolve into coding editor and auditor roles, reviewing and refining what the system suggests.
That dependency on human approval is exactly where CAC starts to show its limits at scale, which we will cover in further sections.
What Is Autonomous Medical Coding?
Autonomous medical coding is an AI-driven process that reads clinical documentation, interprets the full clinical story, applies coding guidelines, and generates complete, compliant ICD-10, CPT, and modifier codes, without requiring a human to review every chart. It uses advanced AI systems that go beyond suggestion and into end-to-end execution.
Autonomous coding solutions typically leverage AI and logic to generate codes automatically and qualify the encounter as “final coded ready” without any human intervention. Further, eliminating humans from interacting with the chart entirely for encounters that successfully complete the process.
How autonomous medical coding works:
- Clinical documentation is pulled directly from the EHR
- NLP and ML models read and interpret the full clinical context
- Codes are assigned, validated, and compliance-checked automatically
- High-confidence encounters go straight to billing — no human review
- Only complex or ambiguous cases are escalated to a human coder
The next frontier: Agentic AI in Medical Coding
The most advanced implementations are now moving beyond autonomous coding into Agentic AI — where the system doesn’t just assign codes but takes sequential, intelligent actions across the revenue cycle. In 2026, AI medical coding automation operates as an agentic control layer inside RCM workflows, coordinating documentation, coding validation, and billing enforcement rather than operating in isolation.
Unlike traditional automation, which follows fixed rules for repetitive tasks, agentic AI can make complex decisions and orchestrate across AI agents to provide more cohesive, seamless automation, thus functioning more like a coworker than a tool. This means automatically cross-checking payer-specific guidelines, triggering claim submissions, and flagging denials for appeal, all within a single automated workflow.
To see how this works in practice, explore Markovate’s AI medical coding software.
Autonomous Medical Coding vs. CAC: Head-to-Head Comparison
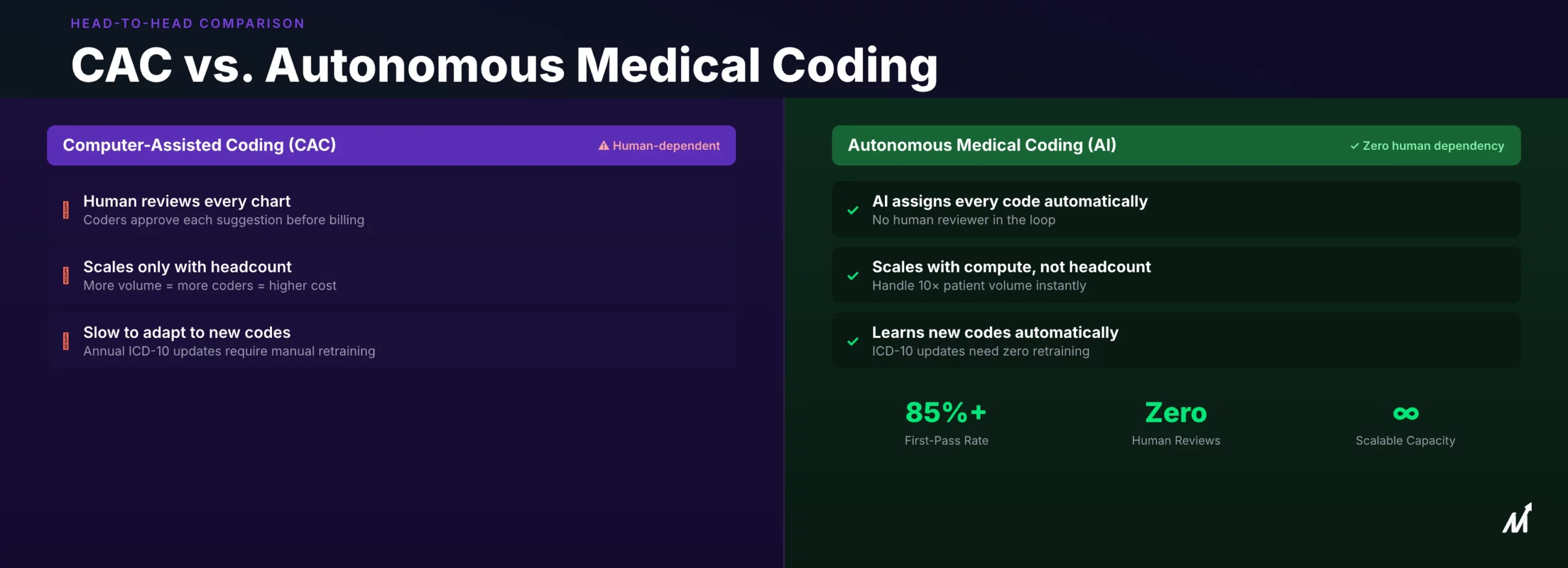
The core difference between CAC and autonomous medical coding comes down to one thing: who makes the final call — a human or the system.
Here is how the two compare across the parameters that matter most to healthcare organizations:
| Parameter | Computer-Assisted Coding (CAC) | Autonomous Medical Coding |
| Human Involvement | Required for every chart | Only for complex/ambiguous cases |
| Code Assignment | Suggests codes, human approves | Assigns and submits independently |
| Processing Speed | Days (pending human review) | Seconds per encounter |
| Accuracy | Varies — struggles with ambiguous clinical language | Upto 95% accuracy |
| Scalability | Limited — requires hiring more coders as volume grows | Scales with compute power — no additional staff needed |
| Payer Rule Updates | Requires manual reprogramming | Adapts and infers new rules automatically |
| Audit Trail | Limited visibility into code rationale | Full explainable audit trail per code assigned |
| Coder Shortage Risk | High — directly dependent on headcount | Low — operates independently of staffing levels |
| Cost Over Time | Increases with volume and headcount | Decreases as the automation rate improves |
CAC was built for a different era — one where coding volumes were manageable, and coder availability was not a crisis. Autonomous coding removes that dependency entirely for routine encounters, freeing human coders to focus on complex cases that genuinely need clinical judgment.
Why CAC Is Hitting Its Limits in 2026
CAC was designed for a simpler coding environment. In 2026, that environment no longer exists. Here are the four pressure points pushing organizations beyond CAC:
1. ICD-10 Update Complexity Is Accelerating
The FY 2026 ICD-10-CM update brought 487 new codes, 38 revised codes, and 28 deleted codes — effective October 1, 2025. Each annual update requires CAC systems to be manually reprogrammed, retrained, and re-validated. For organizations processing thousands of claims daily, that lag creates a direct window for coding errors and claim denials.
2. The Coder Shortage Is Getting Worse
The United States currently faces a 30% shortage of certified medical coders. CAC does not solve this; it still requires a trained coder to review and approve every suggestion. As volumes grow and headcount stays flat, the backlog compounds.
3. Claim Denial Rates Are Rising
Claim denial rates have surged over 20% in the past five years, now exceeding the 10% threshold across many health systems. A significant portion of these denials trace back to coding errors that CAC’s suggestion-and-review model fails to prevent consistently.
4. Coding Complexity Is Outpacing CAC’s NLP Capabilities
Value-based care models require more granular documentation of patient outcomes and comorbidities. CAC systems built on older NLP architectures struggle with this level of clinical specificity — particularly with abbreviations, multi-condition encounters, and complex procedure bundling.
The global medical coding market is projected to grow from USD 8.91 billion in 2025 to USD 14.01 billion by 2030, driven largely by the shift toward AI-driven automation as organizations recognize that human-dependent systems cannot scale with these pressures.
CAC helped organizations move faster than manual coding. But faster is no longer enough; the demand now is for accurate, autonomous, and scalable.
Where Autonomous Medical Coding Solutions Fit
Autonomous medical coding is not a one-size-fits-all replacement for every coding workflow. It delivers the most value in specific settings where volume, speed, and accuracy pressure are highest.
1. High-Volume Hospital Systems
Large health systems processing thousands of encounters daily are the clearest fit. Autonomous coding absorbs routine charts at scale, emergency visits, outpatient encounters, and routine inpatient stays, freeing human coders for complex DRG cases and surgical documentation.
2. Multi-Specialty Physician Groups
Practices managing multiple specialties face wide variation in coding complexity. Autonomous systems handle high-frequency, lower-complexity encounters autonomously while escalating specialty-specific edge cases to the right coder — reducing bottlenecks across the board.
3. RCM Outsourcing Organizations
Revenue cycle management companies handling coding for multiple provider clients benefit significantly. Autonomous coding increases throughput without proportional growth in headcount, directly improving margins and turnaround-time commitments.
4. Organizations With High Denial Rates
If claim denial rates are consistently high, coding errors are likely a contributing factor. Autonomous systems with built-in payer rule validation and audit trails address this at the source, before claims are submitted.
5. Practices Facing Coder Turnover
With medical coder turnover at historic highs, practices that rely heavily on individual coders carry significant operational risk. Autonomous coding reduces that dependency and keeps coding velocity stable regardless of staffing changes.
It is worth noting that autonomous coding works best as a hybrid model, not a full replacement. Complex cases, rare diagnoses, and high-risk encounters still benefit from human review. The goal is to let the system handle what it handles well, and surface only the exceptions that genuinely need a coder’s clinical judgment.
Markovate’s AI Medical Coding Software
Markovate’s AI medical coding software is built for healthcare organizations managing high coding volumes, complex documentation, and evolving compliance needs.
The solution analyzes patient notes, procedures, and diagnoses in real time — automatically predicting and extracting ICD-10 and CPT codes using proprietary AI trained on extensive medical datasets. It understands full clinical context, validates documentation, and flags missing or incomplete codes, acting as an intelligent co-pilot for coding teams.
Key capabilities include:
- Intelligent Code Prediction & Mapping — Real-time ICD-10 and CPT code suggestions with validation and gap flagging
- High-Volume Batch Processing — Simultaneous processing of thousands of encounters with consistent accuracy
- AI Medical Scribe Integration — Real-time voice transcription fed directly into the coding engine
- Real-Time EHR Integration — Seamless connection with existing electronic health records
- Audit-Ready Output — Full compliance with CMS, Medicaid, and HIPAA standards
Designed for health systems, hospitals, physician groups, RCM firms, and medical coding companies, the platform supports teams across clinical, billing, and health IT environments without disrupting existing workflows. In fact, organizations using Markovate’s solution have seen significant reductions in coding costs and faster claim processing cycles. Additionally, coding accuracy improves consistently over time — all while maintaining full HIPAA and CMS compliance from day one.
Conclusion
CAC was a meaningful step forward in medical coding, but it was built for a different scale, a different level of complexity, and a different era. In 2026, with coder shortages widening, payer rules evolving faster, and coding volumes growing across every care setting, waiting for human approval on every chart is no longer a sustainable workflow.
That said, autonomous medical coding addresses this directly — not by removing coders from the equation, but by redirecting their expertise where it matters most. Routine encounters get processed accurately and instantly. Meanwhile, complex cases get the human attention they deserve.
As a result, for healthcare organizations evaluating whether to move beyond CAC, the question is less about whether autonomous coding works. Instead, it is about finding the right implementation partner who understands both the clinical and technical sides of the problem.
Talk to Markovate’s team to discuss what autonomous medical coding can look like for your organization.



